 | Glaucoma: What Every Patient Should Know |  |
|---|---|---|
| Previous Section | Next Section |
| Glaucoma: What Every Patient Should Know | |
|---|---|---|
| Previous Section | Next Section |
There are a variety of other surgical procedures for glaucoma to treat glaucoma, some of which have been tested for 10 years and others that are newer. These have become very frequently performed, especially in combination with cataract surgery, so a vast experience is being produced recently. They range from variations in operations that have been in use for a long time to those that use relatively new concepts and devices. Our treatment of glaucoma was greatly benefited by development of trabeculectomy and tube-shunt surgery, so further improvements or additional choices for particular situations will be valuable.
The newer operations to be considered are the FDA-approved procedures that all share the feature that they work by trying to get the aqueous humor out of the eye better to lower eye pressure. A term that has been applied to some of these is minimally invasive glaucoma surgery (MIGS). All require at least one or more incisions in the eye and some include the permanent implantation of artificial devices in the eye. As yet, the consensus of many experts is that one or more of these procedures will find a place to treat milder glaucoma with surgery when only a modest lowering of eye pressure is needed. Some have been compared to cataract surgery’s eye pressure lowering in trials where some eyes get the cataract surgery alone and some eyes get the new procedure and cataract surgery. None has been compared head to head with each other, nor to trabeculectomy, for example.
The newer glaucoma operations can be divided into 3 main groups, based on their approach. One group of procedures (“angle surgery”) surgically alters the trabecular meshwork (where aqueous flows out), typically by removing it along part or all of the whole circumference of the inner eye to reduce the resistance to fluid outflow. This can be done with a double edged blade or a bent needle (called goniotomy). Or, other procedures with the same type of approach thread a suture or a device behind the meshwork, run them all around to the starting point, then pull to break through the entire meshwork (OMNI, Trab 360, iTrack, GATT). These are actually similar to procedures that have been successfully used in children with glaucoma, called goniotomy and trabeculotomy (see section Children and glaucoma). The success rates in achieving eye pressure lowering for these angle procedures are largely reported in patientswho were treated by the techniques, but without a randomly chosen comparison (control) group. Their potential advantage over trabeculectomy or tube-shunt surgery would be the lack of dysfunctionally low eye pressure or later infection. Of course, early infection from the time of initial surgery would be possible. The time during which instruments are placed into the eye is substantially longer than with trabeculectomy or tube-shunt, so the term “minimally invasive” may be overstated. Repeated later bleeding from the meshwork has occurred with this group of procedures.
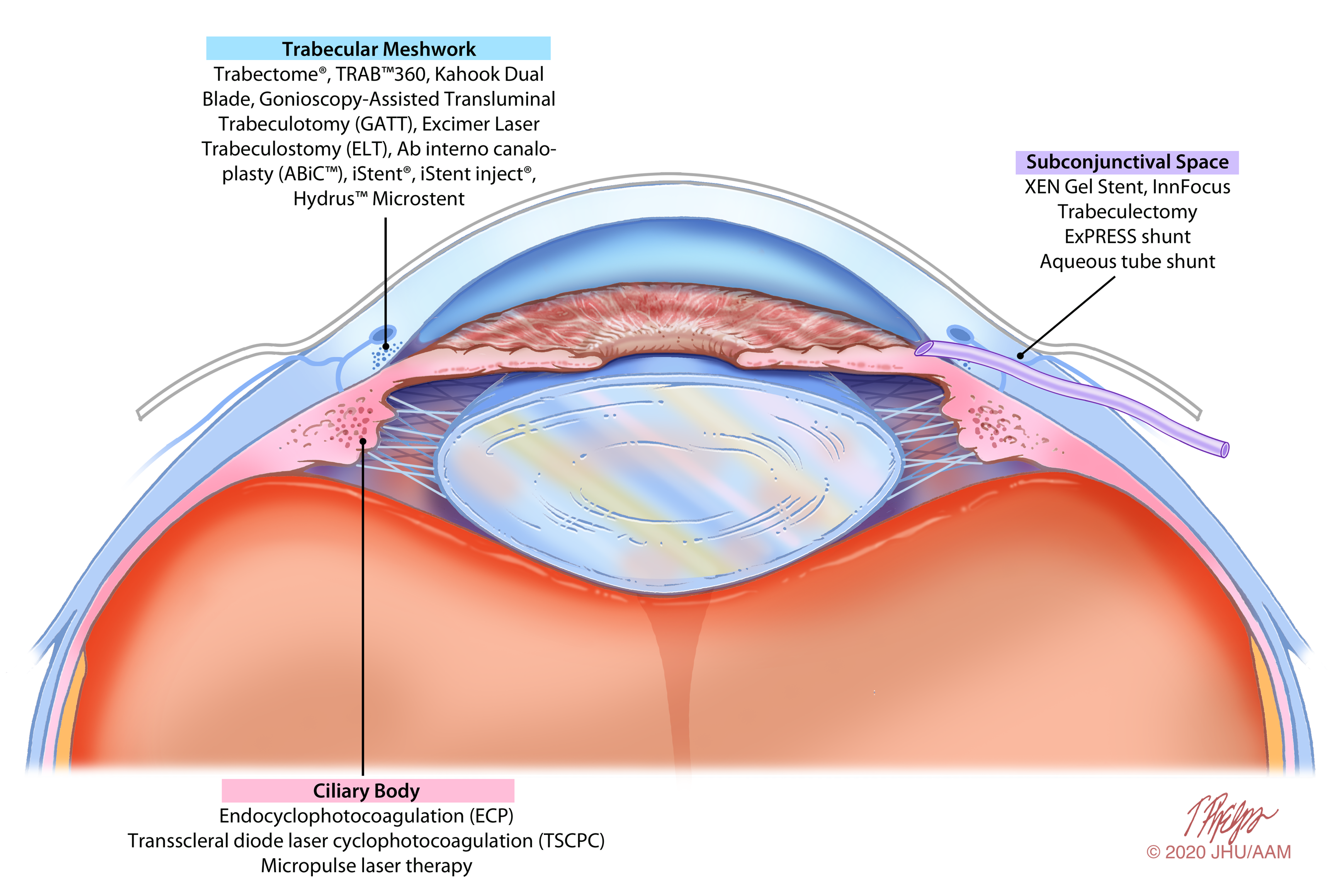 |
A second group of procedures places a device into the meshwork to attempt to improve outflow (iStent, Hydrus). These stents made of metal inserted into the trabecular meshwork with the concept that the opening in the stent will provide an outflow channel to lower eye pressure better. The FDA has only approved these surgeries for patients who are also undergoing cataract surgery at the same time, and in each case the initial results suggested that the stent gave significantly lower eye pressure than cataract surgery alone, though more of the effect was due to the cataract surgery. The pressure lowering effect of Hydrus has been shown to last for 5 years and its effect was better than versions of the iStent in a randomized trial comparing the two. Inserting stents adds a few minutes to cataract surgery. All materials in eye surgery devices are safe for an MRI scanner and you would not set off the TSA metal detector. There have been no reported problems with this group of devices eroding out of the eye, falling out of place, or causing damage to the eye otherwise, so their safety level is very good. Such was not the case for a device called CyPass, which was also an artificial tube-like device placed at cataract surgery, but into the space between the two layers called choroid and sclera with its open end in the front chamber of the eye. Like the other stents, it was intended to lower eye pressure, but by letting aqueous out through the uveoscleral pathway. Approved in 2016 by the FDA, it was removed from use by the company in 2018 when the data began to suggest that damage to the cornea was occurring in eyes with CyPass, potentially leading to a need for corneal replacement in the future. This stresses the need to monitor the safety and effectiveness of new (and old) procedures for glaucoma.
A final type of newer surgery involves placement of a tube-like device into the front chamber of the eye and leading aqueous humor to exit under the conjunctiva (XEN and PreserFlo MicroShunt). They differ from the tube-shunt because they don’t have a reservoir to accept the aqueous, so they often have a bleb, like trabeculectomy. Both devices require opening the conjunctiva and making an opening into the eye, though typically no iris hole is made. In a direct, randomized comparison trial of MicroShunt to trabeculectomy, the success rate of trabeculectomy was better. The XEN device is made of porcine gelatin, so if you have religious beliefs that restrict you from having medical devices that are derived from pigs implanted in your body, you should have a conversation with your religious leader. Unlike trabeculectomy, the pressure with XEN or MicroShunt cannot be adjusted in the early postoperative period, as there are no adjustable sutures. When the pressure is not controlled adequately, reoperations called needling are done, sometimes more than once to improve the chance of success with the two procedures.
If you would like to support the cost of providing and maintaining this book with a charitable donation of any size, please click here.