 | Glaucoma: What Every Patient Should Know |  |
|---|---|---|
| Previous Section | Next Section |
| Glaucoma: What Every Patient Should Know | |
|---|---|---|
| Previous Section | Next Section |
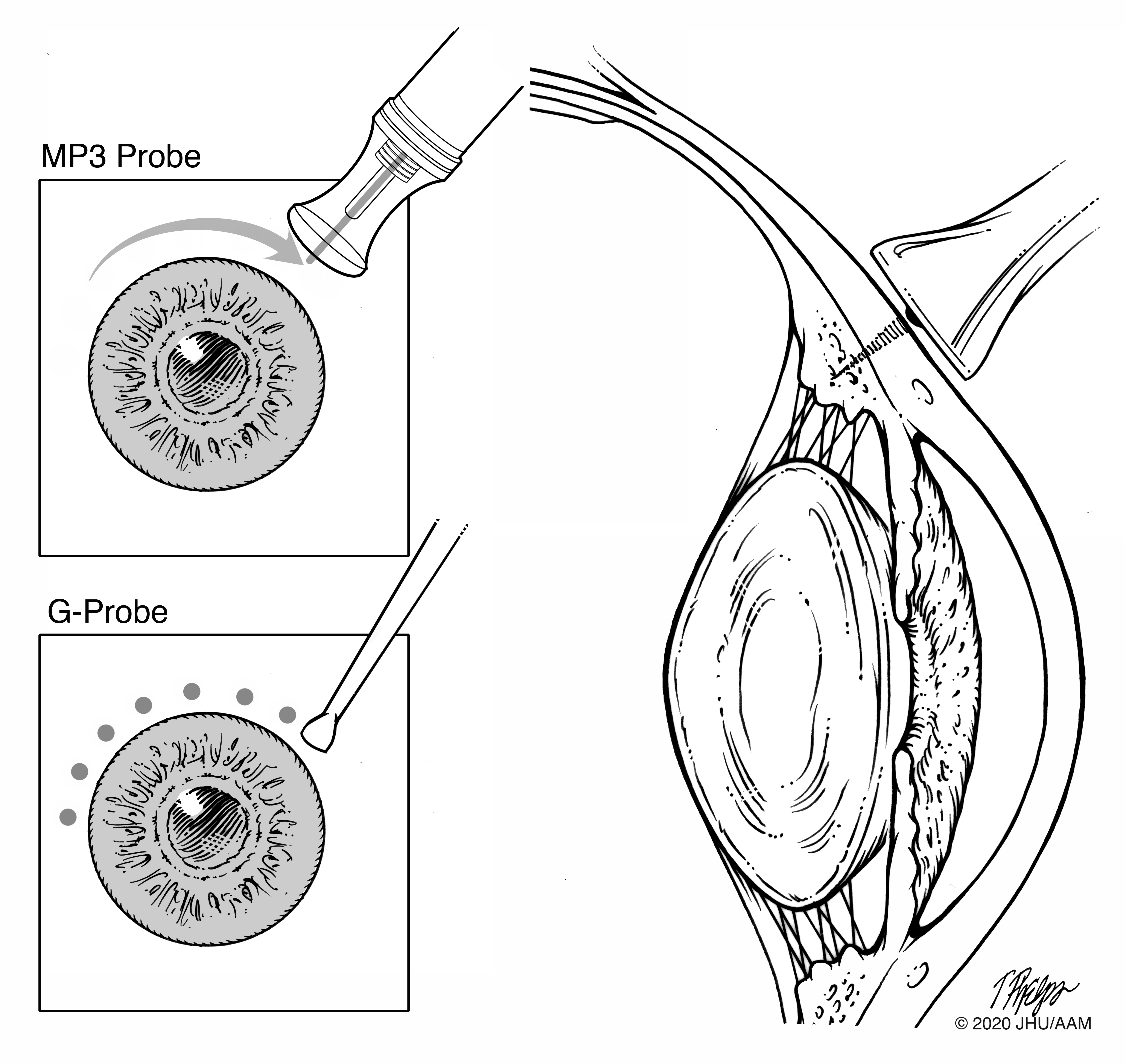
Laser treatment can decrease the amount of aqueous humor that is being formed by the ciliary body. The laser is delivered only in the operating room, due to the pain that would be caused. This is unlike laser angle treatment described above that is done in the office with eye drop anesthesia. The laser can be delivered from the outside of the eye by pressing a probe containing through a fiber optic cable against the outside of the eye. These treatments use a diode laser and are called either trans-scleral diode or micropulse laser treatment, depending upon the way in which the laser energy is configured (Figure 27). Alternatively, the laser can be delivered by a probe that is inserted into the front or the mid-portion of the eye with the viewing done either through the pupil or by an endoscope, that allows the surgeon to see where the laser will deliver on a TV screen. In general, the laser treats the tissue of the part of the eye that produces aqueous humor (ciliary body), which decreases how much fluid is being made and subsequently lowers eye pressure
 |
The treatment, especially the one done from the outside of the eye, is quick (about 10 minutes), but trans-scleral diode ciliodestruction has been most often reserved for those glaucoma eyes in which neither trabeculectomy nor tube-shunts would work well. This is because the treatment causes damage inside the eye, releasing parts of the destroyed tissues into the central cavity of the eye where they cause inflammation and debris that must settle down and be engulfed before vision is back to what it was before surgery. Furthermore, eyes that have had this treatment sometimes develop swelling in the central vision area, the macula, and reading vision can be affected. Rarely the laser can lead to a very low eye pressure that can stay that way permanently. But, when major pressure lowering is needed and other treatments haven’t worked, trans-scleral diode ciliodestruction can save vision. When the target is not achieved, a repeat laser treatment can be done, treating more of the fluid-producing area. Sometimes there is more pain after this treatment than the other glaucoma surgeries.
A recent change was made in how laser can be delivered to the ciliary body from the outside, using an on and off alternating laser light (micropulse). The concept, which has been widely used in treatment of other diseases, is to obtain a good laser effect, but not to produce explosive or large damaging effects, while still achieving a controlled pressure. The treatment requires substantial local anesthesia and is done in a surgical suite. There have been no randomized trials of micropulse laser compared to diode ciliodestruction, nor to other procedures. The initial series of reported patient groups show modest complications, but its potency is still being evaluated by changing the amount of laser delivery. Eyes with severe glaucoma have been reported to have a combination of the micropulse standard treatment and a version of trans-scleral diode ciliodestruction combined, so its advantage in that setting is questionable.
The other mode of laser delivery to decrease aqueous production is endocyclophotocoagulation (ECP). Its major advantage is that the surgeon can see the effect of the laser delivery on the ciliary body processes as it is given, so the right amount and no more is used. It requires that the patient be locally anesthetized in the operating room, and the endoprobe must pass into the eye through at least one incision and sometimes two, depending on how much treatment is to be given. The procedure is nearly always done only in eyes that have had cataract surgery in the past, or, are having cataract surgery with ECP combined. The eye that still has its lens (cataract) in place does not allow enough room to get the probe in place. Again, it may be most useful for mild glaucoma eyes, as the more poorly controlled eyes have been reported to require more extensive surgery combined with ECP. There have been no controlled clinical trials of ECP compared to either cataract surgery alone or compared to any other glaucoma surgery. This procedure produces inflammation in the eye and may be a poor choice for eyes with an inflammatory condition (uveitis; see section Secondary glaucoma).
If you would like to support the cost of providing and maintaining this book with a charitable donation of any size, please click here.