 | Glaucoma: What Every Patient Should Know |  |
|---|---|---|
| Previous Section | Next Section |
| Glaucoma: What Every Patient Should Know | |
|---|---|---|
| Previous Section | Next Section |
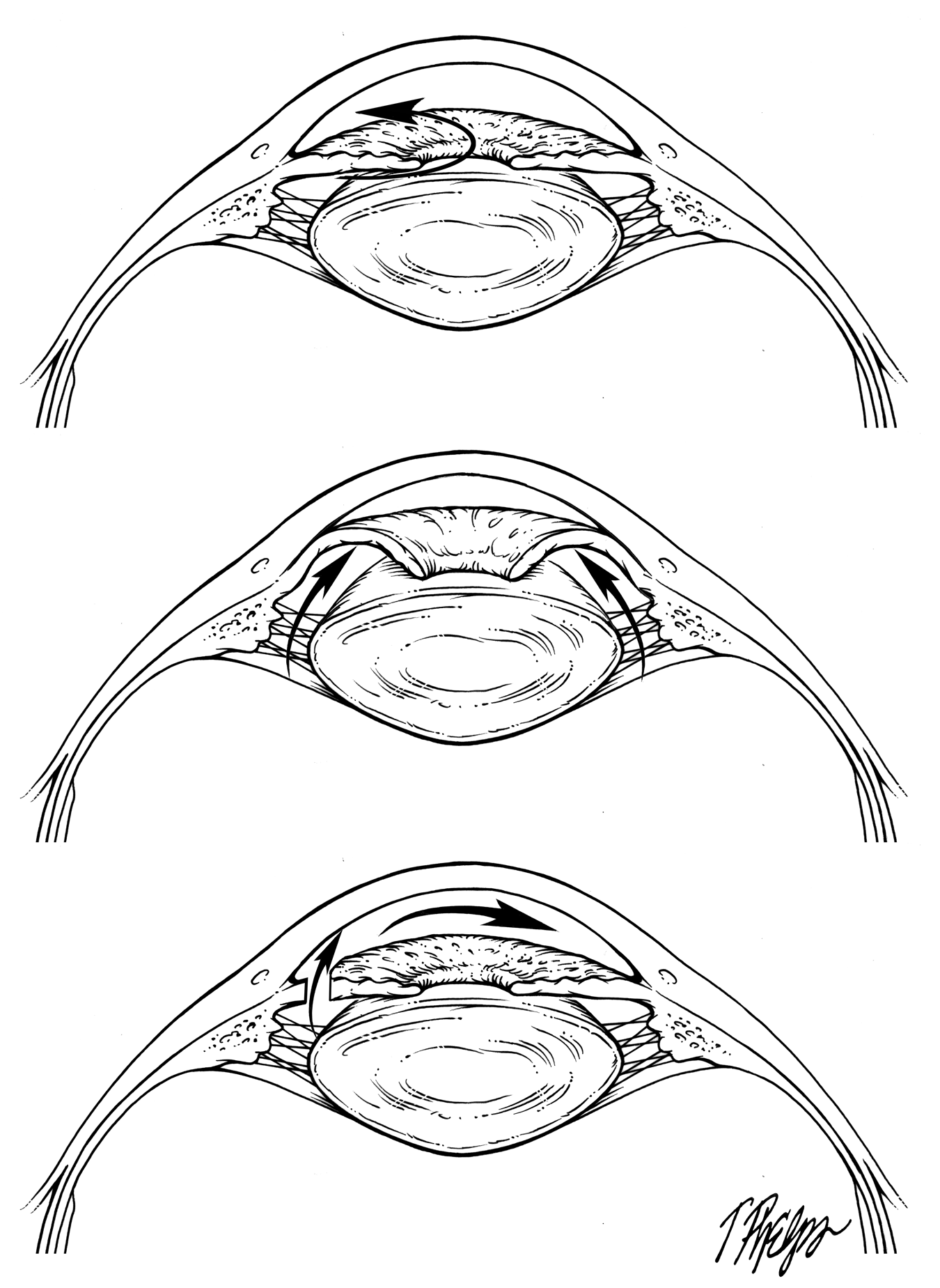
Normally, aqueous humor moves from the back chamber of the eye into the front chamber of the eye, after which it goes back into the blood stream. (People often confuse this with tears that are outside the eye—aqueous humor is only inside). To move from back to front, aqueous must pass between the iris and the lens and through the pupil opening (Figure 7). Angle closure eyes are generally smaller in all dimensions than average. The passageway is very narrow in smaller eyes and the fluid can get blocked in trying to move through. This is known as pupil block. In angle closure glaucoma, the iris is so close to the trabecular meshwork that when pupil block increases, it pushes the iris against the meshwork, blocking the outflow of aqueous humor. The lens in angle closure eyes is also more forward (meaning it is closer to the cornea), increasing the difficulty for aqueous humor to pass between the lens and iris on its way to the anterior chamber. When this resistance is very high (more pupil block), the pressure behind the iris is greater than in front of it, making the iris billow forward like a sail in a strong breeze. If this forward iris movement carries it to the point of closing the angle, drainage is blocked, and eye pressure rises.
 |
The increase in eye pressure in angle closure eyes can be intermittent and moderate, or less commonly, sudden and drastic. This sudden increase is called an acute angle closure crisis or attack. Acute angle closure is actually uncommon, happening only in a minority of all those with angle closure, but is an emergency, as it can lead to severe, permanent vision damage in days if not treated promptly (see section Acute angle closure crisis). People who have an acute crisis can also rapidly develop haziness in the lens (a condition called cataract) and sometimes need glaucoma surgery to resolve the elevation of eye pressure, even after a laser treatment (see section Operations for glaucoma).
Typical symptoms of an acute angle closure crisis are eye pain, nausea, headaches, halos around lights, and severely blurred vision. Sudden acute angle closure attacks are more likely to occur when the pupil is partially dilated, for example, being in a darkened room such as a movie theater, or when pills or eye drops are taken that dilate the pupil. Dilation refers to a reaction of the pupil that occurs when it increases in size. Drugs that can cause this to occur will have a warning on the label. This can also happen to persons at risk for angle closure when they have an eye exam in which the pupils are dilated with eye drops. Acute angle-closure crisis is a true emergency, for which immediate eye exam and treatment are vision-saving. Emergency room medical personnel should always check eye pressure in persons with severe headache, since acute attacks can be so severe that the whole head hurts. The pain makes some people nauseated and their vomiting is occasionally misinterpreted as an acute abdominal problem.
As mentioned above, some medications can initiate acute angle closure crisis by dilating the pupil, including cold tablets and pills taken for urinary incontinence. The FDA marks these as potentially dangerous for those with “glaucoma,” but fails to mention that this is only true for persons with angle closure (not those with open angle glaucoma). The treatment for these attacks is a laser procedure called a laser peripheral iridotomy. The laser creates a hole in the iris, so that blockage of aqueous humor no longer occurs. Angle closure patients who have had laser iridotomy can take these types of medications and have their eyes dilated without risk.
Based on research conducted by Glaucoma Center of Excellence researchers at Johns Hopkins, there are a number of other features of the eye’s behavior that contribute to angle closure and angle closure glaucoma. These are considered in the next section (How did you get glaucoma?) However, it is a good idea to make a laser iridotomy for several groups:
Those with signs that the angle is closing such as headaches and eye pain
Those with closed angles who have an eye pressure higher than normal
Those that have an acute angle closure crisis
Those in whom the angle closure has caused glaucoma (structural and functional damage to the ganglion cells and optic nerve head)
Those who frequently need to use anti-histamine medications
Those who live in or who frequently travel to places where they don’t have access to eye care providers
Description of laser iridotomy, the initial angle closure treatment, is presented in the section Laser glaucoma surgery: iridotomy and angle treatment.
If you would like to support the cost of providing and maintaining this book with a charitable donation of any size, please click here.